

Table of Contents
ToggleTreatments & Expertise

Is Your Child At Risk For Developmental Hip Dysplasia?
Early diagnosis of developmental hip dysplasia in newborns is crucial for effective treatment, Dr. Qureshi specializes in identifying and managing newborn developmental hip dysplasia to ensure your child’s healthy development. Schedule a consultation today to take the first step toward optimal care for your child’s orthopaedic health.
Ensure early diagnosis and the right care
Developmental Hip Dysplasia: Overview
- Developmental hip dysplasia, also known as congenital hip dysplasia or simply hip dysplasia, describes a hip joint where the bones are not aligned properly.
- It is a spectrum condition with a mild form where the hip joint socket is slightly shallow, to the most severe form with complete hip joint dislocation.
- It is one of the most common conditions treated by Pediatric Orthopedic Surgeons, with 1 in 500 infants presenting with a completely dislocated hip.
- Treatment for hip dysplasia in newborns is often challenging because the condition is usually “silent” with no pain early on.
- If left untreated, hip dysplasia can lead to pain and arthritis when the child is older.
- Hip dysplasia treatment depends on the age at which it is diagnosed. Earlier diagnosis leads to better outcomes.
Is My Baby At Risk Of Hip Dysplasia?
Babies are at an increased risk of hip dysplasia in the following situations:
- There is a family history of hip dysplasia
- The baby was in a breech position at the time of birth
- Multiple pregnancies, such as twins
However, many babies born with hip dysplasia do not have any of these risk factors. Hip dysplasia is more common in girls than boys. Hip dysplasia is more common in firstborn children than in later pregnancies.
How Do You Diagnose Hip Dysplasia?
Most newborn babies will have a physical examination by a doctor to look for hip dysplasia. However, even by expert doctors, hip dysplasia can be difficult to diagnose on clinical examination. An ultrasound scan is recommended if there are any concerns from the physical examination or if the baby has any risk factors. In babies older than 4 months, an ultrasound scan may not adequately visualise the hips, and a pelvis X-ray may be more useful.
Some countries conduct universal screening, while others follow a selective approach. In selective screening, imaging is only done if risk factors or exam abnormalities are present.
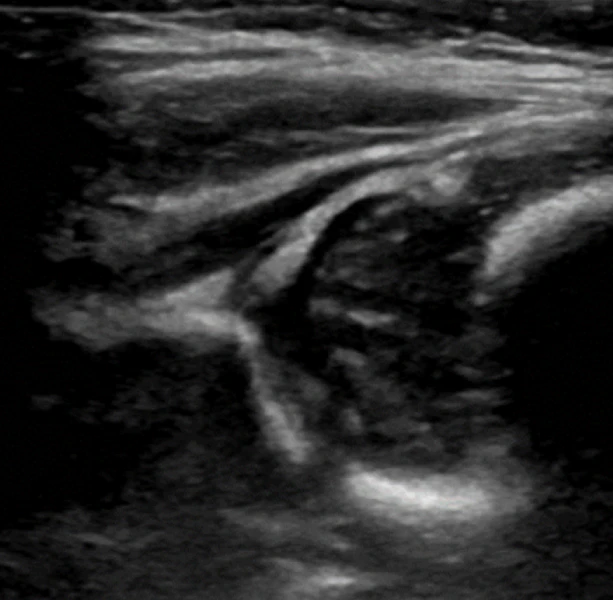
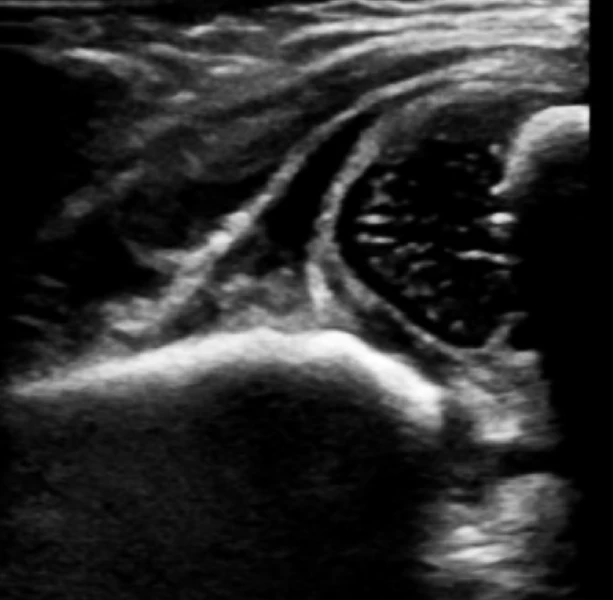
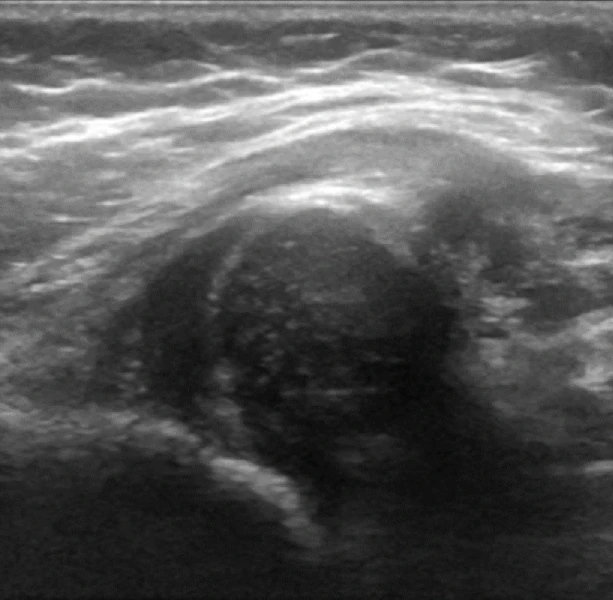
How Is The Ultrasound Scan Done?
The baby is placed in a specialised cradle that allows them to comfortably lie on their side while the upper thigh can be scanned with the ultrasound probe. The scan is undertaken by a sonographer, and the images are interpreted in real-time by Dr. Qureshi, a pediatric orthopedic surgeon in Dubai. Three factors judge the quality of the hip on ultrasound:
- Where is the ball about the socket? The ball should sit deeply in the socket and should not “bob” in and out when the leg is moved. If the ball is not in the socket, it is dislocated.
- Is the socket “roof” covering the ball of the hip joint horizontally? The alpha angle is an important measurement in the ultrasound scan. It measures the angle of the roof. The angle should be more than 60 degrees. The socket will likely be shallow if the angle is less than 60 degrees.
- Does the socket roof adequately cover the ball of the hip joint? The socket should cover more than 50% of the ball.
In many babies, the scan may show mild instability or reduced socket coverage when done earlier than 6 weeks. In such cases, it may be useful to repeat the scan in two weeks to see if there is any improvement in the baby’s natural growth rather than starting treatment for hip dysplasia in infants immediately.
Request an Appointment to Consult with Dr. Assad Qureshi
How Do You Treat Hip Dysplasia In A Baby?
Treatment for hip dysplasia in infants often involves non-surgical methods. They have a good chance of the hip being placed back into the joint using a brace or harness to hold the legs in a position that puts the ball back in the socket. Harness treatment aims to keep the hip stable and allow the ligaments and socket to become more stable with growth. Many different devices are available, but the most common one for hip dysplasia treatment is the Pavlik harness.
The Pavlik harness is a simple device that parents can be shown how to apply. It consists of:
- A wide strap that goes around the chest and is held comfortably under the arms by shoulder straps. The chest strap has red and blue tagged straps to connect to each of the boots.
- A soft boot for the right foot marked with a red tag (R for red, R for right)
- A soft boot for the left foot is marked with a blue tag.
The treating doctor will outline the treatment program:
- The Pavlik harness is typically worn for 23 hours daily until the hip is stable on ultrasound.
- The harness may need to be worn for 6 to 12 weeks.
- Follow-up ultrasound scans at 2-6 weekly intervals are used to monitor the progress of the treated hip and decide when the harness treatment is complete.
In many cases, this approach is successful and avoids hip dysplasia surgery.
What If The Dislocated Hip Does Not Correct With The Harness?
If the ultrasound scan after two weeks of harness use shows that the hip is still dislocated and will not come back into the joint, then it is advisable to discontinue harness treatment. In this case, the doctor may recommend a hip dysplasia surgery, which involves gently repositioning the hip joint. This recommendation may also be made if the child is over 6 months of age at the time of diagnosis and it is felt that the harness is unlikely to be effective.
How Is A Closed Reduction Under Anesthesia Done?
- The procedure is done in an operating theatre as the child needs to be given a general anesthetic to ensure they are completely relaxed.
- A needle is inserted under X-ray guidance into the hip joint to inject some dye. This is called an “arthrogram.”
- The arthrogram outlines the shape of the ball and socket in the hip joint.
- The arthrogram is used to determine if structures around the hip block the ball from entering the socket.
- An attempt is made to place the ball deeply into the socket and see if it remains stable with mild movement. This procedure is known as a closed reduction of the hip joint.
- The baby is then placed into a hip spica plaster cast, which holds the legs in the correct position to keep the ball stable while the hip matures and becomes more stable.
- A CT scan is done a few days after the closed reduction to confirm that the hip has remained in the joint and has not slipped out again.
- The spica cast usually lasts 6 weeks to 3 months until the hip is stable.
- If the hip cannot be placed back into the joint using a closed reduction, the hip should not be forced in but left dislocated. The surgeon will then discuss the need for a surgical procedure known as open reduction to place the hip back into the joint. This is usually done when the child is a little older.
If you’re concerned about your child’s hip development or need expert guidance, contact Dr. Assad Qureshi for comprehensive hip dysplasia treatment in Dubai.