Table of Contents
ToggleTreatments & Expertise

Developmental hip dysplasia, also known as congenital hip dysplasia, is a condition in which the hip joints and the bones are not aligned properly. The severity of this condition can vary, ranging from slightly shallow hip joints to complete dislocation of the hip joint. This condition is extremely common, with 1 in 500 infants experiencing severe hip dysplasia.
Get expert care for late-diagnosed DDH.
How Do You Diagnose Hip Dysplasia?
Hip dysplasia can first be discovered by the parents when their child starts walking with:
- Asymmetric Creases: Parents may notice an extra thigh or buttock crease, indicating leg shortening.
- Hip Clicking: You can hear a click at the hip joint due to the hip popping in and out of joint.
- Limited Range Of Motion: Parents may also notice that when they change the nappies, one leg moves more freely than the other.
- Limping: The asymmetry caused by the hip dislocation can cause the child to walk with a painless limp. The child may sway or have a “bobbing” gait due to one leg being shorter when they walk. If both hips are dislocated, there may not be any leg length difference, but the child will often walk with a waddling gait.
How Do You Confirm A Diagnosis Of Hip Dysplasia?
If there is any suspicion of hip dysplasia, imaging studies are required to confirm the diagnosis. An ultrasound is done, as the hip is mainly cartilaginous, which does not show up on X-ray. In children older than 6 months, X-rays are more useful to detect if the hip is dislocated and whether the socket is shallow.
The features that are looked for on the X-ray include:
- Osific nucleus: The ball of the hip joint changes from cartilage to bone, becoming visible on the X-ray. If the hip is dislocated or subluxed, the bone appears later than expected.
- Steep Roof: As the child grows, the roof of the socket should become more horizontal. If the hip is dysplastic, the socket roof remains steep.
- Teardrop widening: The teardrop is the inner floor of the socket. If the hip is correctly jointed, as the child begins to walk, the ball pushes deeper into the socket, making the teardrop become thinner over time. In dysplastic hips, the teardrop remains wide.
How Do You Treat A Dislocated Hip In A Walking-Age Child?
A closed reduction under general anaesthetic can be attempted, but is usually unsuccessful in older children. This is because the structures in the hip act as barriers to the ball being placed back into the socket. Our paediatric orthopaedic surgeon in Dubai recommends open surgery to remove them and place the ball into the socket. If the ball is not in the socket, the socket does not develop and remains shallow. If the ball is placed into such a socket, it can easily slip out and dislocate again. Over time, the ball may grow big if it is outside the socket. Trying to keep a big ball in a shallow socket can be quite difficult with a plaster cast.
What Are The Surgical Steps In Treating A Dislocated Hip In A Walking-Age Child?
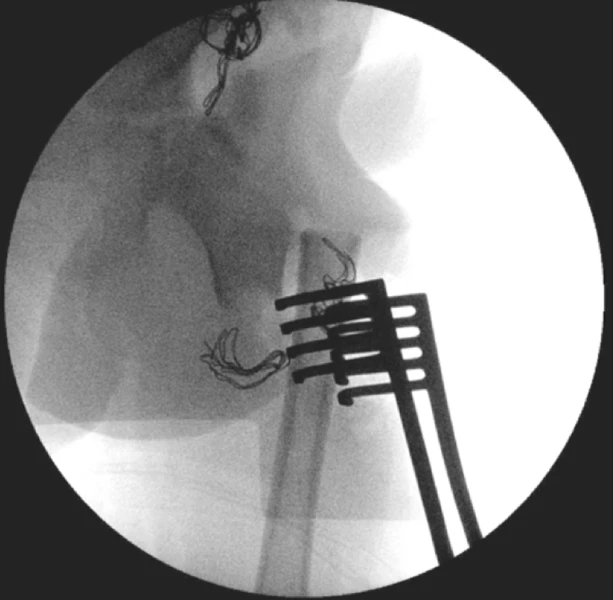
- Arthrogram: A special dye is injected into the hip joint to help the surgeon see any blockages and check how well the hip socket can hold the ball of the joint.
- Adductor release: Tight groin muscles are loosened to make it easier to fit the ball back into the hip and reduce harmful pressure on the joint.
- Open reduction: The hip is carefully opened through surgery so that any tissue blocking the joint can be removed, allowing the ball to be placed properly in the socket.
- Femoral osteotomy: The thigh bone is shortened to relieve stress on the hip and help the legs match in length and movement.
- Pelvic osteotomy: The pelvic bone is reshaped and adjusted to better cover and support the hip joint, often using a piece of bone from the femur.
- Spica cast application: A full lower-body cast is applied to protect the hip and leg and help everything heal in the correct position.
How Long Will My Child Be In the Hospital?
Usually, patients stay about three days, including pre- and post-surgical treatment of developmental dysplasia of the hip. The surgery is undertaken on day one, after which the child is admitted to the ward in a plaster cast with an epidural infusion for comfort and a urinary catheter for ease of nursing. On day two, blood tests are done to check if a blood transfusion may be required, and the epidural is continued for comfort. On day three, the epidural and catheter are removed, and the child has a CT scan to confirm the hip is appropriately relocated. If this is satisfactory, the child is discharged from the hospital for care to continue at home.
What Are The Risks Of Surgery To My Child?
DDH surgical treatment is categorised as major surgery due to the duration and complexity of the procedure. Surgical risks include general risks from any major surgical intervention and risks specific to surgery for hip dysplasia.
General risks include:- Need for blood transfusion: It is not uncommon for children to require a blood transfusion either during or after surgery if both a femoral and a pelvic osteotomy are undertaken.
- Nerve or vessel injury: This is a very rare complication for surgeons who are experienced in hip dysplasia surgery.
- Anaesthetic risks: Anaesthetic reactions are thankfully very rare, and this risk will usually be explained by the anaesthesiologist.
- Infection: This is a very rare complication in this type of surgery, and antibiotics are routinely given before and after surgery to mitigate this.
- Redislocation: Although the accepted risk of redislocation is 1 in 10 patients, an experienced surgeon should have a much lower rate of redislocation than this.
- Proximal femoral growth disturbance: This is where progressive changes to the ball of the hip joint are thought to have arisen from the surgical insult. This risk is very specific to individual surgeons, and a paediatric orthopaedic surgeon should be able to tell patients how often and the severity of when they have encountered this in their practice.
- Residual dysplasia: This is where the socket fails to develop adequately despite the hip being in the joint and is evidenced by a socket remaining shallow as the child grows older. This risk is very specific to individual surgeons and depends on whether the first surgery sufficiently corrects the shallow socket to enable normal development.
How do I know if the surgery was successful?
The outcome of developmental dysplasia of the hip (DDH) treatment is only known much later, when the child is older. Young children will not have pain from a dislocated hip. Similarly, young children will not have pain if there is re-dislocation or residual dysplasia. The best indication of a good outcome in the future is whether the X-rays show that the hip is gradually becoming more normal in terms of a spherical ball that sits deeply in the socket with good roof coverage.
If you are looking for a professional opinion, diagnosis, or DDH treatment in Dubai, contact us today. Dr. Qureshi, a renowned hip dysplasia surgeon in Dubai, has years of experience and expertise in paediatric orthopaedic surgery and has helped numerous patients in his career.
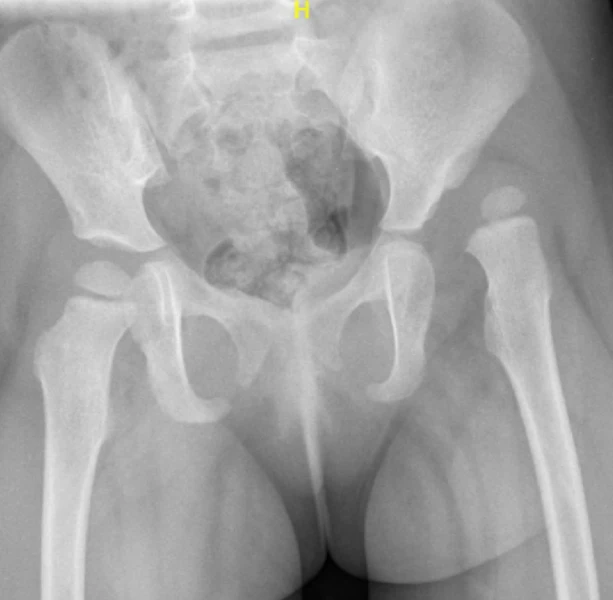
Clinical Case A : 2 year old girl presenting with left dislocated hip


What is the outcome following single-stage hip reconstruction?
According to the International Hip Dysplasia Institute, one in five hundred children is born with a dislocated hip. Although some will be diagnosed at birth, many will evade clinical detection and present when the child is walking age and a painless limp or asymmetry in the legs is noted. In children older than six months, an X-ray is a better investigation than an ultrasound to diagnose hip dysplasia.
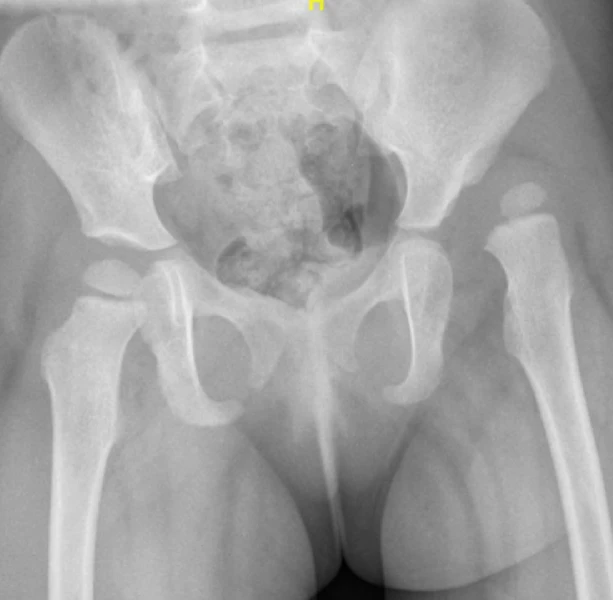
Clinical case B : 2 year old boy presenting with dislocation of both hips




Treatment Options for Hip Dysplasia in Children
Frequently Asked Questions
Do hips dislocate in older children?
According to the International Hip Dysplasia Institute, one in five hundred children is born with a dislocated hip. Although some will be diagnosed at birth, many will evade clinical detection and present when the child is walking age and a painless limp or asymmetry in the legs is noted. In children older than six months, an X-ray is a better investigation than an ultrasound to diagnose hip dysplasia.
Can we still attempt a closed reduction?
If the hip is found to be dislocated on X-ray, a closed reduction under general anaesthetic with hip spica application can still be attempted. However, the chances of success reduce with the advancement of patient age.
What are the challenges in treating a late presenting hip dislocation?
The challenge with late presenting hip dislocation is often more than the fact that the ball of the hip joint is not in the socket. The other issues frequently encountered are:
- Barriers to the hip being relocated through manipulation: This is often due to structures being interposed between the ball and socket preventing its relocation.
- Deformity in the femur (thigh bone): Although the leg may be shorter, frequently the thigh bone overgrows and often may not point in the right direction.
- Deformity in the acetabulum (socket): In the absence of the favourable biomechanical influences of the normal hip joint, the empty socket fails to develop and remains shallow.
How does Dr. Qureshi treat late presenting hip dislocation?
Dr. Qureshi passionately believes in correcting all elements of the deformity as well as relocating the hip joint. His favoured approach for late presenting hip dislocation in walking-age children ,that does not respond to closed reduction, is single-stage hip reconstruction. Single-stage hip reconstruction is a comprehensive surgical procedure that addresses all elements of the deformity in late presenting hip dislocation. The key elements are
- Arthrogram (dye study) to outline the anatomy of the joint and determine whether a closed reduction is feasible.
- Open reduction procedure where the joint is opened to address the factors obstructing the hip from going back into the joint.
- Soft tissue balancing where muscles that are contracted are addressed through lengthening to ensure the hip joint is stable.
- Femoral osteotomy procedure where shortening of the thigh bone is done to help equalize leg lengths and the rotational alignment is also corrected to make the hip joint more stable.
- Pelvic osteotomy procedure, which is usually the most crucial element of maintaining a stable hip and minimising the risk of redislocation by dividing the pelvic bone to bring the socket down to improve coverage of the hip.
- Hip Spica cast, a plaster cast is applied from the upper abdomen down to the ankles leaving the nappy area relatively accessible for hygiene purposes.
What is the outcome following single-stage hip reconstruction?
Surgical outcomes for late-presenting hip dislocations are typically associated with the age of diagnosis, with less favorable results reported for older children in the literature. Dr. Qureshi employs a single-stage hip reconstruction technique, addressing all deformity elements comprehensively rather than solely focusing on hip relocation. Dr. Qureshi is pleased to showcase successful cases treated with this advanced approach.
According to the International Hip Dysplasia Institute, one in five hundred children is born with a dislocated hip. Although some will be diagnosed at birth, many will evade clinical detection and present when the child is walking age and a painless limp or asymmetry in the legs is noted. In children older than six months, an X-ray is a better investigation than an ultrasound to diagnose hip dysplasia.
If the hip is found to be dislocated on X-ray, a closed reduction under general anaesthetic with hip spica application can still be attempted. However, the chances of success reduce with the advancement of patient age.
The challenge with late presenting hip dislocation is often more than the fact that the ball of the hip joint is not in the socket. The other issues frequently encountered are:
- Barriers to the hip being relocated through manipulation: This is often due to structures being interposed between the ball and socket preventing its relocation.
- Deformity in the femur (thigh bone): Although the leg may be shorter, frequently the thigh bone overgrows and often may not point in the right direction.
- Deformity in the acetabulum (socket): In the absence of the favourable biomechanical influences of the normal hip joint, the empty socket fails to develop and remains shallow.
Dr. Qureshi passionately believes in correcting all elements of the deformity as well as relocating the hip joint. His favoured approach for late presenting hip dislocation in walking-age children ,that does not respond to closed reduction, is single-stage hip reconstruction.
Single-stage hip reconstruction is a comprehensive surgical procedure that addresses all elements of the deformity in late presenting hip dislocation. The key elements are
- Arthrogram (dye study) to outline the anatomy of the joint and determine whether a closed reduction is feasible.
- Open reduction procedure where the joint is opened to address the factors obstructing the hip from going back into the joint.
- Soft tissue balancing where muscles that are contracted are addressed through lengthening to ensure the hip joint is stable.
- Femoral osteotomy procedure where shortening of the thigh bone is done to help equalize leg lengths and the rotational alignment is also corrected to make the hip joint more stable.
- Pelvic osteotomy procedure, which is usually the most crucial element of maintaining a stable hip and minimising the risk of redislocation by dividing the pelvic bone to bring the socket down to improve coverage of the hip.
- Hip Spica cast, a plaster cast is applied from the upper abdomen down to the ankles leaving the nappy area relatively accessible for hygiene purposes.
Surgical outcomes for late-presenting hip dislocations are typically associated with the age of diagnosis, with less favorable results reported for older children in the literature. Dr. Qureshi employs a single-stage hip reconstruction technique, addressing all deformity elements comprehensively rather than solely focusing on hip relocation. Dr. Qureshi is pleased to showcase successful cases treated with this advanced approach.