


Patient Presentation
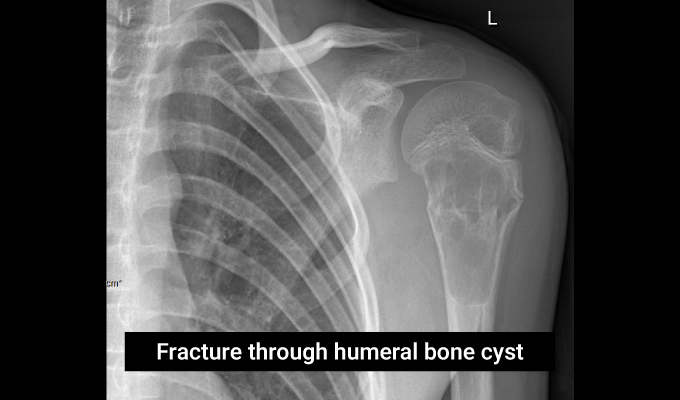
A 12-year-old boy presented with arm pain after a twisting injury during sports. He was seen in the emergency room. X-rays were done, which showed a fracture of the humerus. The fracture occurred in a weakened area of bone due to a cystic lesion. This case was managed by a paediatric orthopaedic surgeon, who specialises in bone and joint conditions in children.
Table of Contents
ToggleIs your child facing an orthopaedic problem?
Diagnosis
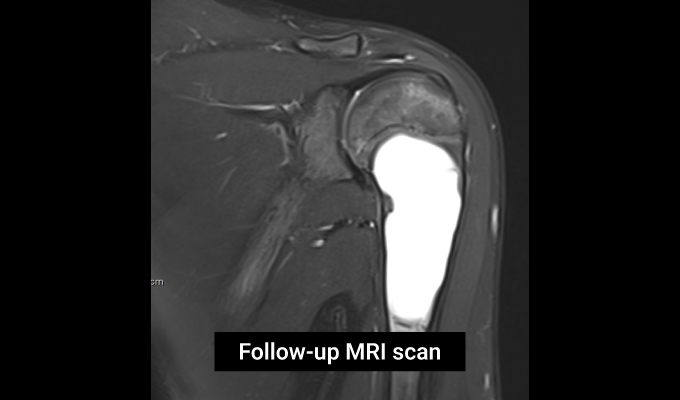
Analysis of the radiographs demonstrated that the fracture had occurred due to weakening of the bone by a cystic lesion within. An MRI scan was arranged to characterise the lesion. The MRI scan revealed the lesion to be a simple bone cyst, also known as a unicameral bone cyst. It is a benign fluid-filled cavity in the bone that often demonstrates a “fallen leaf” sign. It is usually found in the long bones such as the humerus and the femur. They are most commonly encountered in children and teenagers. The exact cause of the cyst is unknown. They are usually asymptomatic and spotted as incidental findings on X-rays done for other clinical reasons. However, active cysts that grow to a large size can weaken the bone within. This can lead to a break in the bone with much less force than what would normally be required. This is termed an insufficiency fracture.
Small cysts may disappear over time and not require any treatment. However, large cysts that remain adjacent to the growth plate are considered active, as they have a tendency to grow. In this case, the cyst was very large and adjacent to the growth plate, indicating an active cyst.


Treatment
A fracture through a cyst can promote bone regeneration within the cyst, restoring the bone to its original strength. In this case, a period of observation was undertaken to see if the fracture would lead to resolution of the cyst. The fracture healed, and six months later, the MRI was repeated. The MRI images demonstrated that the cyst had increased in size and was still adjacent to the growth plate. Given the lack of resolution, a recommendation of surgical intervention was made to the family to treat the cyst and reduce the risk of another fracture.
The aim of treatment is to promote healing of the cyst and strengthen the bone to prevent fracture. However, there is no clear consensus amongst orthopaedic surgeons on the optimal treatment strategy for simple bone cysts. The options vary from minimally invasive techniques to open surgery. The options include:
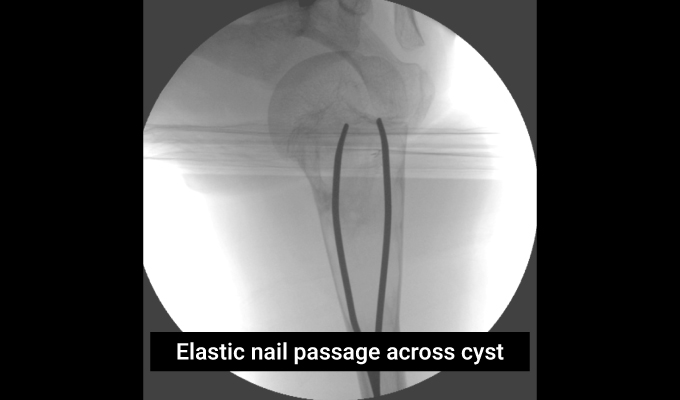
- Intramedullary nailing is a technique where thin, flexible metal rods are introduced into the bone and passed across the cyst to disrupt it and stimulate the bone growth. The metal rods also act to stabilise the bone and reduce the risk of fracture while the cyst heals.
- Aspiration and injection of sclerosant involves placing a needle into the cyst to drain it and then injecting steroids or sclerosant to promote bone regeneration. This is a minimally invasive technique. However, the injection may need to be repeated several times in active cysts for complete healing.
- Cyst debridement and bone grafting is an open surgical procedure to scrape the cyst lining and fill the resulting gap with bone graft to enable it to heal. Although there are high rates of success with this technique, open surgery is considerably more invasive with a longer recovery time compared to other techniques.
The patient’s family had seen four other doctors, all of whom suggested an open surgical approach with removal of the cyst contents and filling with bone graft. The family were discouraged by this, as they wished for quicker recovery, given the boy’s active lifestyle and minimal impact on school attendance. Dr. Qureshi, a paediatric orthopaedic surgeon in Dubai, selected a multimodal treatment plan with reduced invasiveness compared with open surgery. The family agreed to go ahead with this procedure.
Under general anaesthesia, two elastic nails (3mm diameter flexible metal rods) were introduced into the humerus through a small incision above the elbow. The elastic nails were passed across the cyst to disrupt it. They were pre-contoured into a curved configuration to impart stability to the bone. Separately, a bone needle was inserted through the skin directly into the cyst with ultrasound guidance. Fifty millilitres of straw-coloured fluid were drained directly from the cyst until no more fluid could be drawn. A different bone needle was used to take a bone marrow aspirate from the pelvis. Bone marrow aspirate is fluid taken through a needle placed in the pelvic bone to draw off fluid rich in bone-stimulating properties. This fluid was then injected into the bone cyst. Three objectives were achieved – drainage, stabilisation and stimulation. The child was discharged home the same day in a sling for comfort.

Worried about your child’s bone or joint health?
Outcome
The boy was seen in the clinic at 2 weeks with X-rays to confirm satisfactory implant placement and check that the small incisions had healed. X-rays at 6 weeks demonstrated new bone ingrowth into the cyst. They were advised to follow up again in 3 months with repeat radiographs. The child returned to normal function, and the family decided to defer follow-up by several months on the premise that complete cyst resolution may take several months. They presented 10 months following surgery. The child had full function and had returned to sports a few months after his surgery. X-rays demonstrated complete healing of the cyst. He was scheduled for implant removal, which proceeded uneventfully, and was subsequently discharged from the clinic with no symptoms and full function.
If you’re seeking expert care for your child’s bone or joint condition, contact us to schedule a consultation with Dr. Qureshi, a paediatric orthopaedic surgeon in Dubai. And learn more about minimally invasive options for managing bone cysts and fractures in children.

Testimonial
“Thank you so much, Dr Qureshi, for everything you’ve done for our son. We’re truly grateful for your care and expertise throughout this journey. I have to admit, we were incredibly anxious before meeting you. We had already consulted with 4 other doctors, all of whom were quick to suggest aggressive approaches for what was, at the time, a 12-year-old boy. But from our very first meeting, you put us at ease. You took the time to involve us in every step of your thought process, and you were open about consulting with your peers to ensure the best path forward. What truly stood out was your sensitivity to my son’s age and stage of growth. You carefully considered this and recommended a treatment plan that was both effective and far less invasive than what others had proposed. We can’t thank you enough; you’ve made a lasting difference, and we’re so grateful to have found you.”

Dr. Assad Qureshi
Dr. Assad Qureshi is a highly experienced Pediatric Orthopedic Surgeon specializing in musculoskeletal disorders in children. With a focus on early diagnosis and advanced surgical techniques, he is committed to restoring function and improving the quality of life for his pediatric patients.