


Can you treat hip dysplasia without surgery?
Surgery is required to achieve two objectives –
- Remove any obstructions to place the ball deeply into the socket and
- Correct the shallowness of the socket and other factors which might cause the hip to re-dislocate. Therefore surgery is only considered if non-operative techniques can not get the ball into the socket or that the ball can be placed into the socket but keeps slipping out.
Contact Dr. Assad for surgical treatment options for Childhood Hip Dysplasia
What surgical procedures are used to treat the hip dysplasia?
The exact surgical procedure depends on the age of the child, the severity of the hip dysplasia and the arthrogram (dye study) findings. The key techniques include:
- Arthrogram – this is where dye is injected into the hip so that we can determine on the x-ray whether the hip is shallow and whether it is unstable.
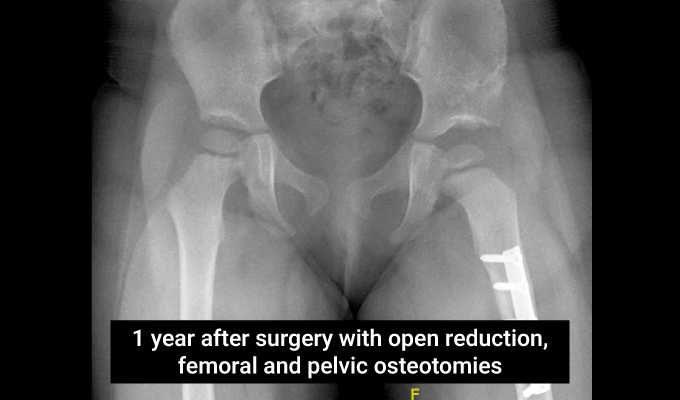
- Open reduction – the hip is opened surgically through a “bikini”incision in the groin crease. Any obstructions preventing the ball from going into the socket are addressed and the ball is taken from the dislocated position and placed into the socket.
- Femoral osteotomy – the femur bone is shortened to minimise pressure on the ball when it is placed in the socket. The ball is made up mainly of cartilage which is soft and easily damaged. Shortening the femur bone reduces the tension in the joint and minimises the risk of the ball being damaged. The bone is fixed with a metal plate and screws. The bone removed from the shortening is used in the pelvic osteotomy.
- Pelvic osteotomy – the socket is re-shaped to make it deeper so that the ball is more stable once placed back inside. This is done by dividing the pelvic bone to lever the “roof” down over the ball so that it can’t dislocate easily. The bone from the femoral shortening is used to fill the gap.
- Capsuloraphy – once the ball is deep in the socket, the capsule is closed over the ball to seal the hip joint and help stop it dislocating.
- Hip spica – a plaster cast is applied over the hips to keep the hip in place while everything heals. The plaster cast (hip spica) is kept on for 6 weeks.
What are the risks of surgery?
General risks of surgery include infection, need for blood transfusion, nerve or vessel injury and risks of anaesthesia. The risk of infection in childhood hip surgery is less than 1% and antibiotics are given during the perioperative period to minimise this risk.
Depending on the scale of surgery some patients may require a blood transfusion during or after surgery. This is usually due to blood loss from the femoral and pelvic osteotomies.
The risk of nerve or major blood vessel injury is less than 1%. Specific risks to the hip during surgery include re-dislocation, avascular necrosis (damage to the ball in the joint) and residual dysplasia (socket remains shallow during development).


Schedule your child’s orthopedic consultation in Dubai today!

Dr. Assad Qureshi
Dr. Assad Qureshi is a highly experienced Pediatric Orthopedic Surgeon specializing in musculoskeletal disorders in children. With a focus on early diagnosis and advanced surgical techniques, he is committed to restoring function and improving the quality of life for his pediatric patients.