


Clinical problem
A 2 week old baby was brought to clinic with a diagnosis of clubfoot by the neonatologists. The pregnancy was unremarkable and the baby was delivered at 38 weeks by caesarean section. There was no abnormality detected on antenatal ultrasound. There was no family history of clubfoot deformity. Newborn examination revealed the left foot resembled a clubfoot and was slightly stiff. The baby was referred to Dr Qureshi for further assessment and treatment.
Table of Contents
ToggleDiagnosis
The baby was seen in the Pediatric Orthopedic clinic. Assessment of the hips did not reveal any obvious instability. Both the feet adopted a clubfoot position. The right foot could easily be stretched out to be straight and point upwards. In comparison the left foot was slightly flexible but could not be brought to point outwards. The ankle was stiff and the foot could not be brought up from its down pointing position. A diagnosis of idiopathic clubfoot was made. An ultrasound of the hips was requested to be done at 4-6 weeks of age to exclude hip dysplasia. After discussion and consent from the parents, the clubfoot was treated using the Ponseti protocol.

Treatment
As the baby’s weight had stabilized, treatment was begun at 3 weeks of age. The Pirani score was calculated at each visit. The Pirani score is a numeric score used to grade various elements of the clubfoot deformity. It’s principal utility is to assess the response to treatment. All clubfeet have high numerical scores on the Pirani score before treatment. The expectation is that the Pirani score reduces over the course of the treatment as each element of the deformity is corrected.
The first cast was applied at three weeks of age in clinic. The first cast corrected the forefoot to match the hindfoot. The cast was applied in two sections. The first section was done after the manipulation and extended from below the knee to the toes. The cast was molded to maintain the foot in the desired position. Once this was done, the second section was applied to extend the cast above the knee. The extension above the knee requires the knee to be bent at a right angle. This angle of the knee is designed to prevent the cast slipping and causing skin problems.
The parents were instructed to look after the cast, look for any signs of slippage and to return in one week. To aid removal of the cast, the parents were advised to soak the cast in a bucket of warm water and to wrap it in a wet towel on the morning of cast removal. The softened cast was easily removed. The Pirani score was undertaken, a manipulation was done to further stretch the foot and the second cast applied. The second cast enabled the foot to be turned outwards in a straight position. A week later the third cast was applied achieving the desired position of the foot pointing out. The Pirani forefoot scores had normalized indicated the forefoot was completely corrected. The baby was scheduled for tenotomy as a clinic procedure the following week.
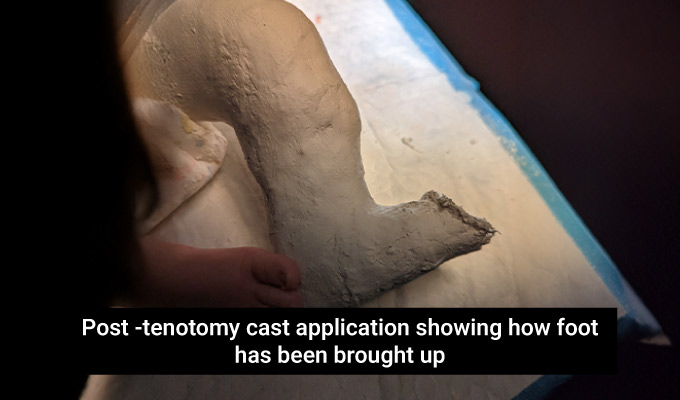
The achilles tenotomy was undertaken in clinic. Local anaesthetic cream was applied to the back of the ankle 30 minutes before the procedure. A small amount of local anaesthetic was injected under the skin to help numb the area. The nurse held the foot in position while the area was cleaned with antiseptic solution. A fine scalpel was passed through the skin in a single pass behind the tendon and then rotated to completely divide the tendon. Complete tendon division was confirmed by easy correction of the foot to point upwards. A final cast was applied in this corrected position for 3 weeks.



Consult Dr. Qureshi, for expert diagnosis and treatment.
Outcome
The cast was removed three weeks after the tenotomy. The feet were placed into the “boots and bar” orthosis which places the foot in a corrected position. Although one foot was treated, both feet need to be in the boots and bar to hold the correction in the treated foot. Instructions were given for the boots and bar to be worn 23 hours a day for 3 months. Typically the boots and bar are removed once a day for bathtime and a bit of a stretch. After three months, the boots and bar were applied for 12 hours a day, usually when the baby was sleeping.
At each follow up, the foot remained nicely corrected. The family returned 1 week after initial boots and bar application to make sure there were no compliance issues and that the baby was comfortable through the night. The next follow up was at 3 months from final cast removal when the boots and bar duration transitioned from 23 hours a day to 12 hours a day. The baby was then seen at 8 months. The foot remained nicely corrected. In the standing position, the foot was straight and pointing outwards. Examination showed that the foot could easily be brought up with no calf muscle tightness. The family were delighted with the outcome and followed up in clinic at scheduled intervals.





Dr. Assad Qureshi
Dr. Assad Qureshi is a highly experienced Pediatric Orthopedic Surgeon specializing in musculoskeletal disorders in children. With a focus on early diagnosis and advanced surgical techniques, he is committed to restoring function and improving the quality of life for his pediatric patients.